I have always been passionate about minimally invasive treatment and now, thanks to the IAS Inman Aligner, I am able to provide an alternative orthodontic solution that is safe, gentle and effective for my patients. Aligning teeth before restoration affords the dentist an opportunity to be minimally invasive, yet able to produce an aesthetic smile that suits patients’expectations. I find the IAS Inman Aligner appliance a very useful tool in achieving this; it is a single, simple appliance both for the dentist and the patient. Plus, it is removable, which encourages patient compliance and is more time-effective than traditional fixed orthodontic brackets.
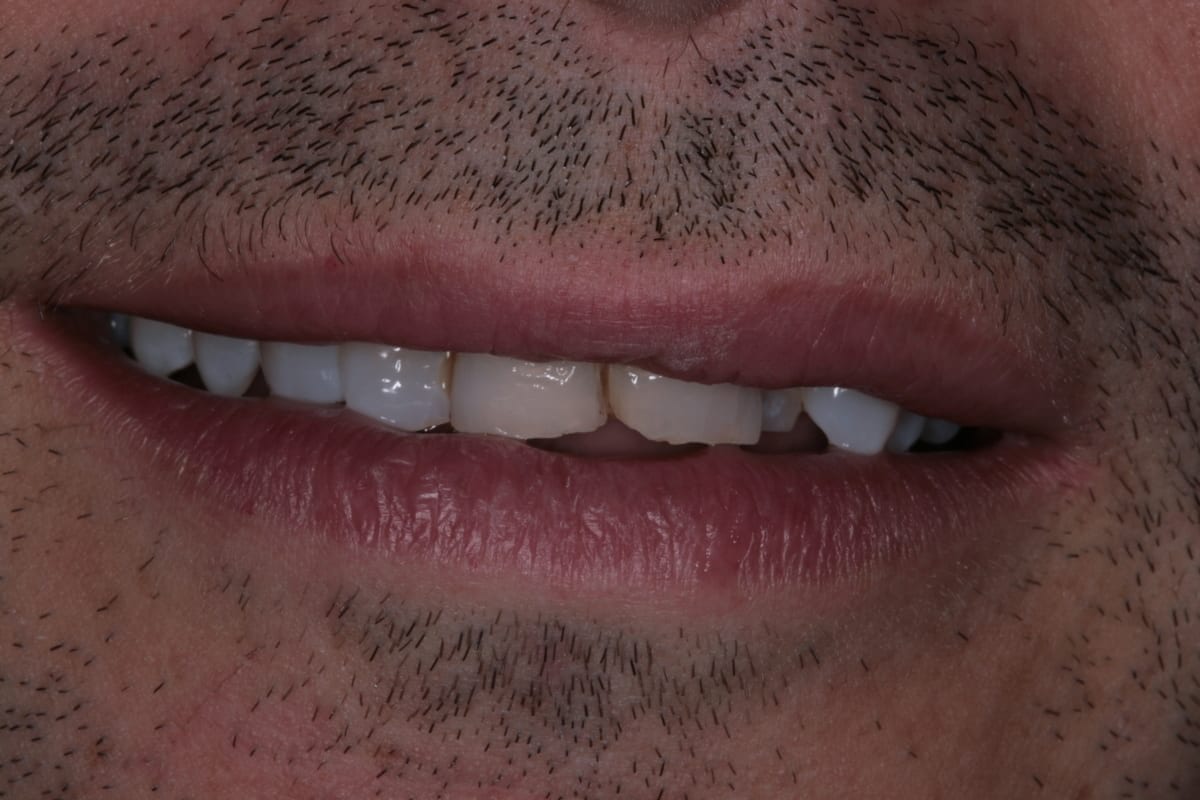
In this case, a 41-year-old male patient presented to the practice to discuss treatment options to correct the appearance of his anterior teeth. The patient’s notes showed that buccal composite fillings had been placed in the past on UR2, UR1, UL1 andUL2–which had become stained and worn–and that he had undergone root canal treatment eight years ago on UR2 as a result of pulpal necrosis. Examination revealed attrition to UR1, UL1, LR2, LR1, LL1 andLL2 with distal caries present inUL1. The patient is a self-confessed tea and coffee drinker, smoker and only brushes once a day.
Orthodontic Assessment
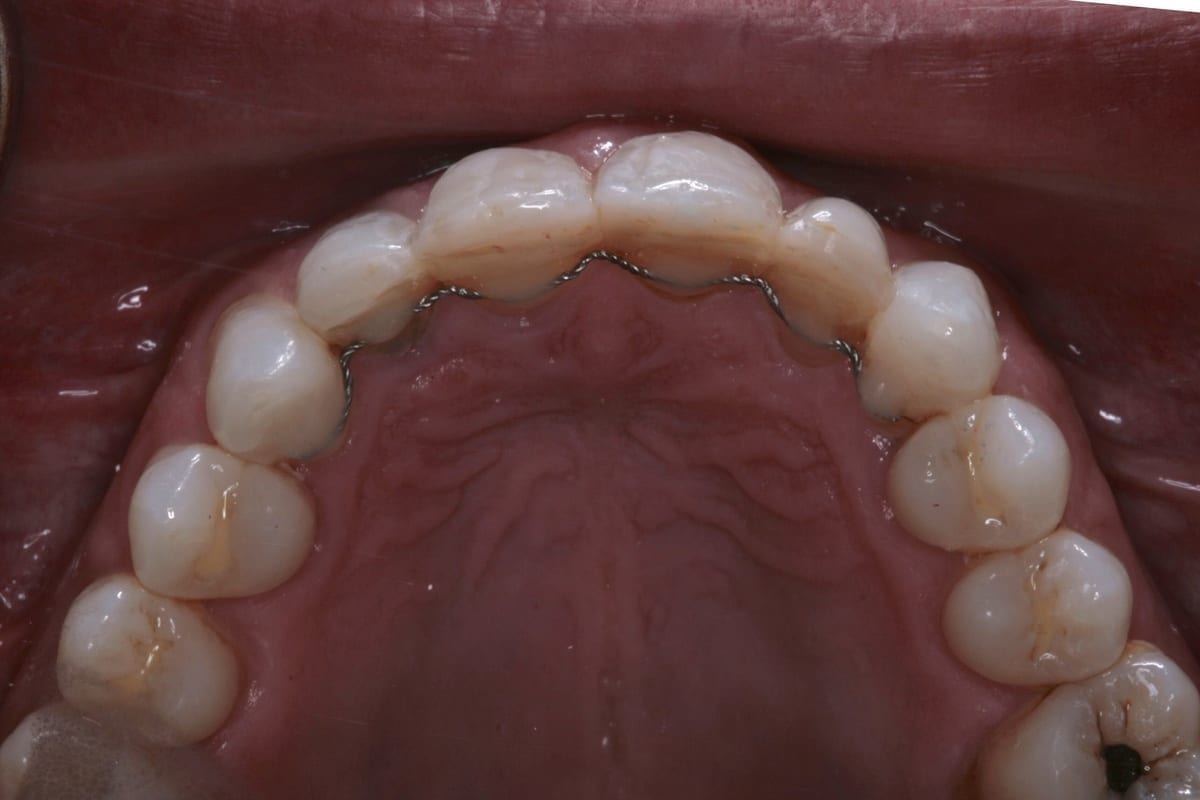
The orthodontic assessment revealed moderate anterior segment crowding in the upper arch with a palatally displaced UL2, distolabially rotated UR2 and a slight labial tilt of UL1. In the lower arch, there was a slight buccal displacement of LL1and mild crowding with a midline shift to the right. (Table 1.)