Demand for adult orthodontics has grown enormously in recent years, with an increasing number of people wishing to straighten their teeth in pursuit of an improved smile. As a result of the various time and financial restrictions faced by many patients today, anterior alignment orthodontics has become particularly popular, offering a safe, highly effective and efficient solution.
Case Presentation
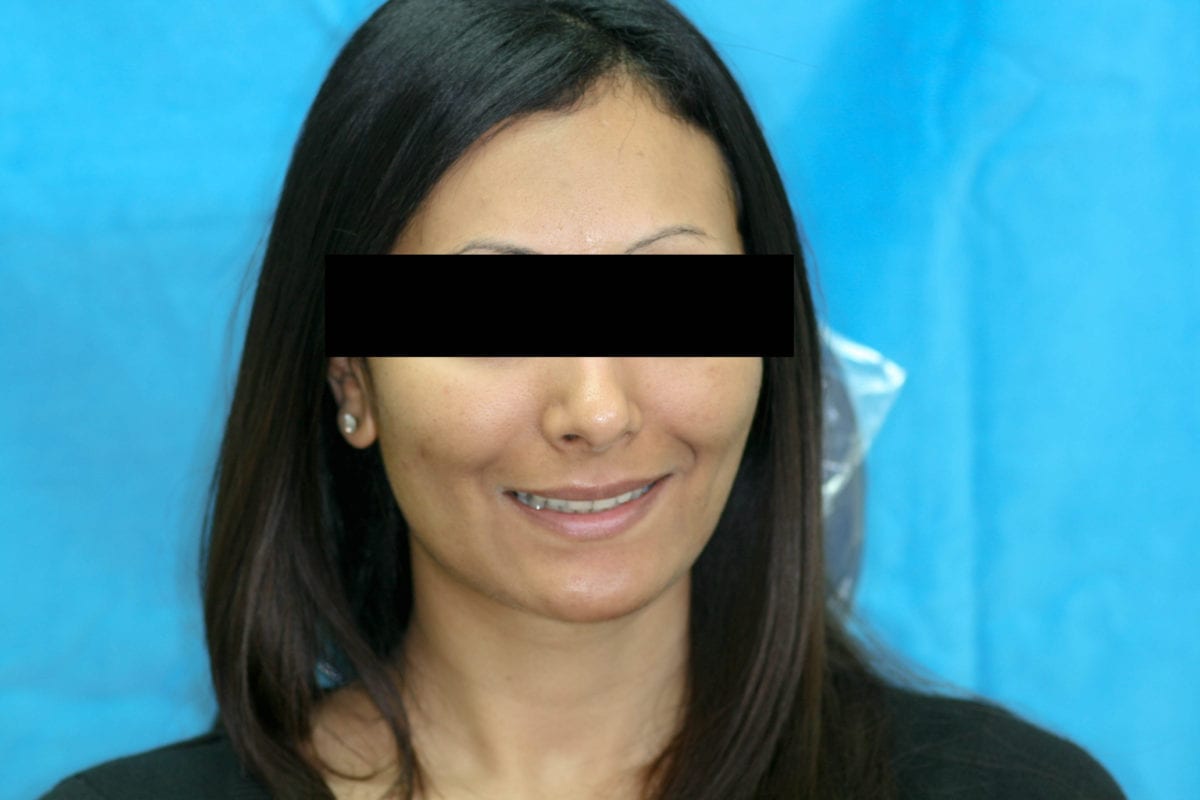
A healthy 33-year-old female presented to the practice with concerns about the appearance of her central incisors – which had become palatally inclined following poor retention after previous orthodontic treatment. Her main intention was to align the anterior teeth, without using fixed braces again. The patient was a non-drinker, non-smoker, regularly attended dental appointments and followed a strict oral care regimen that included brushing twice a day and flossing. Her dental notes also revealed that her upper premolars were extracted at the time of her previous orthodontic treatment.
Orthodontic Assessment
Assessment confirmed good oral health with no signs of periodontitis, though the patient did show signs of discolouration as a result of tea consumption. There were no signs of a crossbite and lips were competent at rest.
An orthodontic assessment was also carried out (see table one).