Helping a Patient Provide Service with a Smile

Treatment carried out by Runeel Joye
Runeel Joye is a general dentist working in a mixed practice in Cheadle. He has been qualified since 2002, graduating from Queen Mary’s University in London. Runeel has been the Principal Dentist at Cheadle Smile Centre since 2012.
A female presented in her early twenties with concerns about the movement of her upper anterior teeth and increasing crowding. The patient presented with Class II division I malocclusion on a Class II skeletal base with an increased overjet, mild upper and lower crowding and deviated upper and lower centre lines. Her oral hygiene was good, though she is a smoker and had a history of taking medication for depression (Fluoxetene).
The patient worked in a public facing role, and was therefore interested in a discreet solution that could solve the problem without being unsightly. Suitability was therefore assessed for treatment with the clear aligners.
| Measurement | Result |
|---|---|
| Skeletal | Class II |
| FMPA | Average |
| Lower Face Height | Lower |
| Facial Asymmetry | None |
| Soft Tissues | Nothing abnormal |
| Overjet | <6mm with proclined upper central incisors |
| Overbite | None |
| Crossbite | None |
| Displacement on Closure | None |
| Incisor Relationship | Class II Division I |
| Molar Relationship | Left: Class I | Right: Class I |
| Canine Relationship | Right: Class II ½ | Left: Class I |
| Teeth Present | 7654321 | 1234567 | 7654321 | 1234567 |
| Centrelines | Upper centre line deviated to the left 1mm | Lower centre line deviated to the right 3mm |
Treatment planning
Photographs and impressions were taken and the Archwize™ digital planning software was used to confirm suitability for treatment with the ClearSmile Aligner. An estimated 1.0mm of interproximal reduction (IPR) would be needed in the maxilla and 1.2mm in the mandible. Tooth whitening was also proposed to complete treatment following alignment. Digital 3D models were created to demonstrate to the patient what could be achieved. With informed consent, we were able to proceed.
Problem list:
- Class II skeletal pattern
- Proclined upper central incisors
- Crowding on the left hand side of both upper and lower arches
- Deviated upper and lower centre lines
- Class II canine relationship on right hand side
- Increased overjet
Ideal treatment aims:
- Correct the skeletal pattern
- Align upper and lower arches
- Align centre lines
- Align incisors and right hand side canines to Class I occlusion
Compromised treatment aims:
- Align upper and lower anterior segments
- Accept deviated centrelines
- Accept canine relationship
Treatment
| Date | Result |
|---|---|
| April 16 | Initial consultation. |
| April 16 | Upper and lower arch impressions taken, photos taken. |
| May 16 | Advised patient that she will need IPR. Clear Aligner consent form signed. |
| June 16 | Composite force drivers placed on first premolars (etch, iBOND adhesive, Venus® Pearl A3) – excess removed with diamond finishing bur. IPR performed on LR2 and LL2 at distal and mesial points using a 0.1mm red diamond strip. Lower arch Clear Aligner fitted. |
| July 16 | Upper Clear Aligner fitted. IPR performed on UR2 and UL2 using 0.1 mm red diamond strip at the mesial and distal contact points. Composite force driver placed on lower left quadrant. |
| August 16 | Impressions taken for the next box of aligners and sent to the IAS orthodontic lab, photos taken. |
| September 16 | Retraction and isolation using an Optragate dam. IPR performed on UR1 and UL1 with 0.2mm IPR strip. Patient started box 2 of aligners. |
| October 16 | Retraction and isolation performed. IPR performed on UR12, UL12, UL3 using 0.1mm red diamond strip. Patient decided that she wants no more treatment on her lower arch. Impressions taken and posted on IAS forum for analysis and discussion. Bonded retainer fitted on the lower arch. |
| November 16 | Retraction and isolation. IPR performed on UR3, UL3 at mesial and distal contact points with 0.1mm red diamond strip and UR1, UR2, UL1 and UL2 at the mesial and distal contact points using a 0.2mm silver diamond strip. |
| December 16 | Retraction and isolation. IPR performed on UL3 contact point using a 0.1mm red diamond strip and UR2 contact point as well as at UR1, UL1 and UL2 using a 0.2mm strip. |
| January 17 | Course of treatment finished, however, UL2 could use more rotation – further Clear Aligners suggested. Patient accepted. Composite drivers removed. Photos taken. Whitening gel supplied and first of additional aligners fitted. |
| March 17 | Retraction and isolation. IPR performed with 0.2mm diamond strips on the UR2, UL2 and with 0.3mm strips on the UL1, UR1 and UL3 contact points. Photos taken, impressions for upper retainers taken. |
| June 17 | Patient happy with appearance of uppers. LL3 position discussed – more aligners suggested. Patient accepted. Upper and lower impressions taken and sent to the IAS lab. Additional lower aligner fitted. |
| August 17 | IPR performed with 0.2mm blue diamond strip on LL2, second additional lower aligner fitted. |
| September 17 | Patient happy with outcome so result acceptance form completed. Impression taken for lower retainer and results sent to the IAS lab. |
Support Utilised
The IAS Academy instructors offered support through multiple stages of the treatment via the online forum. By posting impressions and photographs I was able to benefit from the advice of the experts and other professionals, helping to achieve the best end results.
Case Self-appraisal
Upon reflection, the LL3 would have benefitted with further correction earlier in the treatment process. I only discussed this with the patient at the completion of the upper arch, which delayed treatment slightly following occasional missed appointments. However, treatment with clear aligners fully met the patient’s expectations, achieving a smile she was happy with by using a minimally invasive technique.
 Pre treatment anterior
Pre treatment anterior  Post treatment anterior
Post treatment anterior  Pre treatment anterior retracted
Pre treatment anterior retracted  Mid treatment anterior retracted
Mid treatment anterior retracted  Post treatment anterior retracted
Post treatment anterior retracted  Pre treatment right
Pre treatment right  Post treatment right
Post treatment right  Pre treatment left
Pre treatment left  Post treatment left
Post treatment left  Pre treatment right lateral
Pre treatment right lateral  Mid treatment right lateral
Mid treatment right lateral  Post treatment right lateral
Post treatment right lateral  Pre treatment left lateral
Pre treatment left lateral  Mid treatment left lateral
Mid treatment left lateral  Post treatment right lateral
Post treatment right lateral 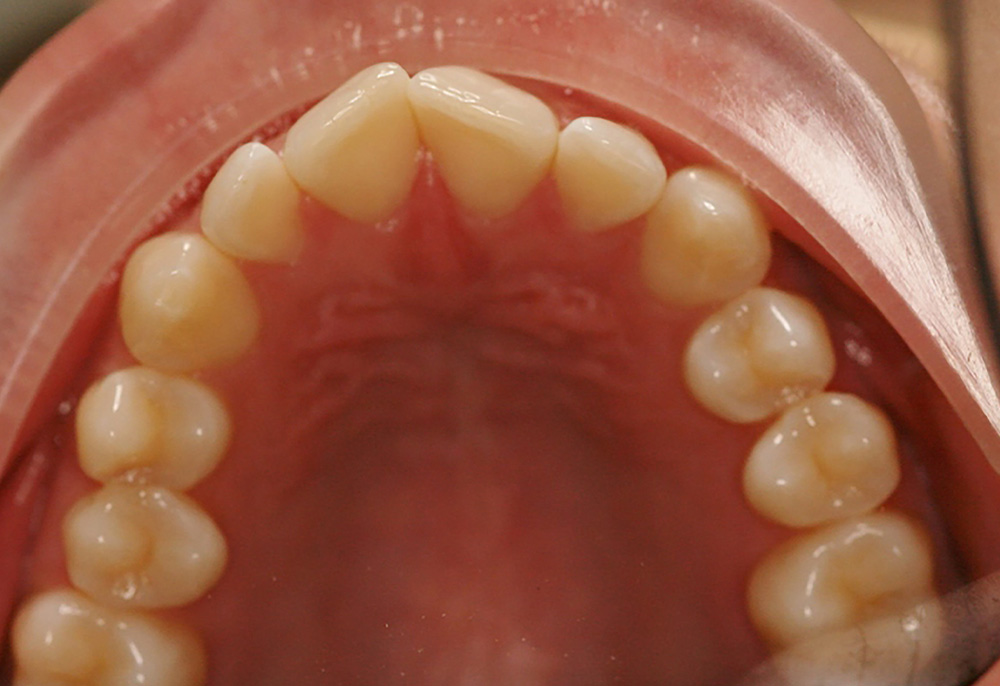 Pre treatment upper occlusal
Pre treatment upper occlusal  Mid treatment upper occlusal
Mid treatment upper occlusal  Post treatment upper occlusal
Post treatment upper occlusal  Pre treatment lower occlusal
Pre treatment lower occlusal  Mid treatment lower occlusal
Mid treatment lower occlusal  Post treatment lower occlusal
Post treatment lower occlusal 
