A 33-year-old female patient presented with concerns about lower crowding, which was affecting her ability to clean her teeth and her smile aesthetics.
Orthodontic Assessment
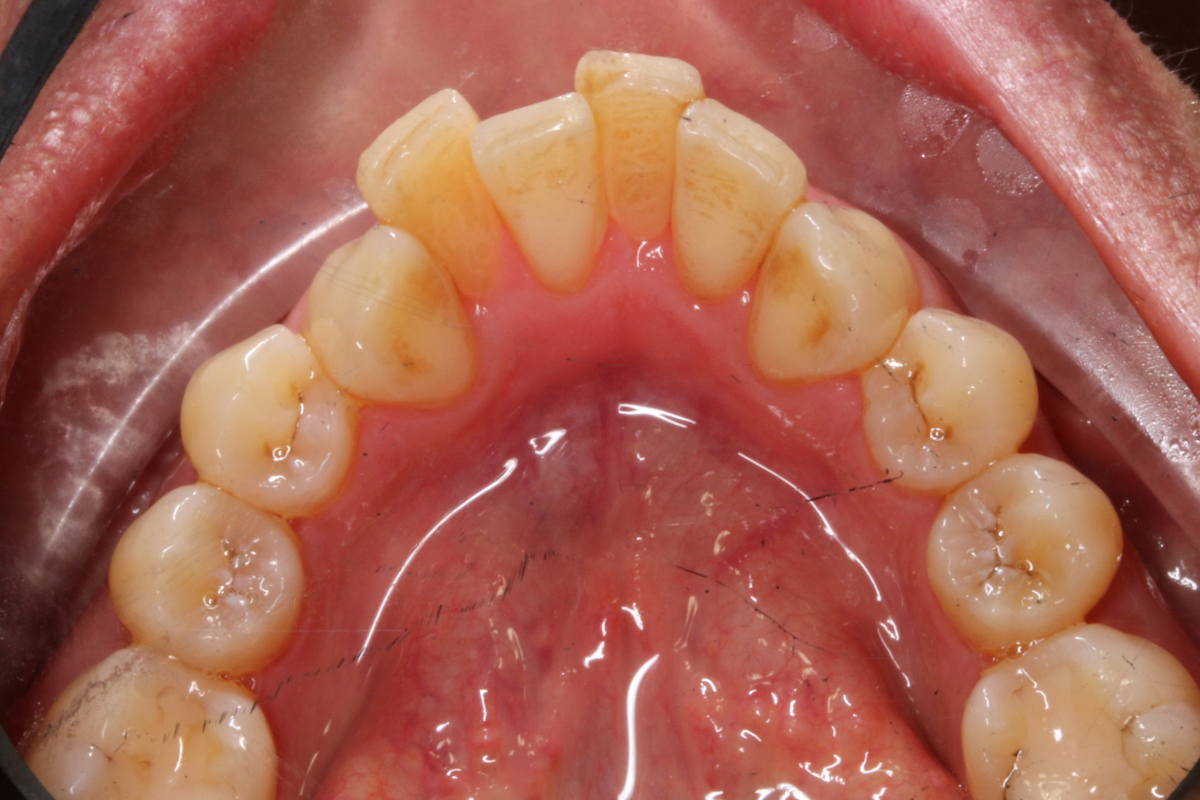
A comprehensive clinical examination was performed (Table 1), revealing a Class II Div I incisor relationship with a reduced overbite on a Class II Skeletal Base and low FMPA. Moderate lower crowding and a thin gingival biotype were recorded, along with 2mm buccal recession on the LL1.