Anterior Alignment Orthodontics for a Relapsed Orthodontic Case
Treatment carried out by Hanmeng Ma
Hanmeng Ma is a general dental practitioner working in a mixed practice in South Woodford.
CONTACT INFORMATION
Woodford House Dental Practice
162 High Road,
Woodford Green
Essex
IG8 9EF
Tel:020 8504 2704
Visit website
Minimally invasive aesthetic dentistry has always appealed to me. Like many others, I began by using composite to explore the many ways I could improve the shapes of teeth. However, there came a point where this was not enough and I realised that to avoid enamel reduction I had to change the position of the teeth. I decided to attend a ClearSmile Inman Aligner course by Dr Tif Qureshi in 2016 and was attracted to the IAS Academy ethos he presented. As a result, I became more interested in Anterior Alignment Orthodontics (‘AAO’), coming to see it as an essential skill in providing minimally invasive dentistry. Subsequently, I completed both the ClearSmile Aligner and ClearSmile Brace courses provided by IAS Academy.
Stepping into orthodontic treatment as a GDP previously scared me a little. I had apprehensions about not knowing enough and not providing the best possible treatment for my patients. IAS Academy teaches a comprehensive assessment procedure that allows treatment to be provided only if the patient is suitable for GDP care. The Archwize™ digital planning procedure is an essential part of the process, as it allows the treatment plan to be checked by yourself, the patient and the experienced advisors on the support forum.
Case presentation
This patient had braces when she was 14 years old but her teeth had relapsed. She was unhappy with the appearance of the upper and lower incisors, and she felt the laterals were inset in her mouth. She had been a regular patient at the practice and demonstrated good oral hygiene. She was also medically fit and led a very healthy lifestyle.
Orthodontic assessment
After a consultation explaining the benefits and limitations of AAO, the patient chose to go ahead with an assessment for the ClearSmile Aligner, as opposed to being referred to an orthodontist. The IAS Academy assessment protocol was followed. Clinical photographs and impressions were taken of the teeth so the laboratory could carry out the Archwize™ planning. (Figures 1-X)
Planning
This patient was suitable for the IAS Academy protocol of non-extraction based orthodontic treatment. A combination of very mild proclination and interproximal reduction (IPR) would be used to create space. The Spacewize+™ digital planning application was used to determine that the lower arch required 1.5mm of interproximal reduction, which was inside the 6mm limitation of the device. Due to the proclination of the lateral incisors on the upper arch, no IPR would be required here. (Figures x-x)
Assessment
A full orthodontic assessment was performed. The TMJ and radiographic report were clear.
| Measurement | Result |
|---|---|
| Skeletal | Mild Class II |
| FMPA | Average |
| Lower Face Height | Average |
| Facial Asymmetry | Present |
| Soft Tissues | Competent lips, average smile line |
| Overjet | 3mm |
| Overbite | 25% |
| Displacement on Closure | None |
| Incisor Relationship | Class II Division I |
| Molar Relationship | Left: Class I | Right: ¼ unit Class III |
| Canine Relationship | Left: Class I | Rights: Class I |
| Teeth Present | 87654321 | 12345678 | 87654321 | 12345678 |
| Centrelines | Lower centreline – coincident | Upper midline – deviated to right by 1.5mm |
Problem list:
- Mild skeletal Class 2
- Molar relationship ¼ unit Class 3 on RHS
- Mild crowding upper and lower
- Increased overjet with a Class 2 div 1 incisal relationship
- Deviated centerline on the upper teeth
Ideal treatment aims:
- Correct skeletal relationship
- Correct molar, canine and incisor relationships to Class 1
- Torqueing of root and crown to ideal angulations
- Reduce overjet
- Relieve upper and lower arch crowding
Compromised treatment aims:
- Relieve upper and lower anterior crowding only
- Accept the skeletal, molar and canine relationships
- Accept possible increased overjet post treatment
- Accept upper midline deviation
The resulting treatment plan involved upper and lower aligners to upright the canines and premolars slightly, and to relieve upper and lower crowding. The Archwize™ analysis from the laboratory suggested a total of 9 upper and 12 lower aligners and the patient was advised to wear one a week. Tooth whitening and composite bonding on the distal edge of the LR2 was discussed with the patient to optimise aesthetics. Finally, fixed upper and lower retainers, as well as Essix retainers for nightwear were planned to ensure retention.
The patient was happy to accept the slightly increased overjet and the deviated centerline. She was not concerned about the posterior bite that resulted from the orthodontic treatment she’d had when she was younger and she understood that AAO offers only anterior teeth alignment. Had the patient not been happy with these compromises, she would have been referred to an orthodontist.
Treatment
In order to monitor the patient closely, short appointments were booked weekly, which allowed me to perform any IPR required and take photographs when appropriate. When lower alignment was completed, a bonded retainer was fitted and an Essix retainer provided for night time.
After the prescribed 9 upper aligners, although that patient was happy with the result, the UR3 needed a little more buccal rotation to achieve a better outcome and the patient was very happy to go ahead. New impressions were taken for the laboratory and they prescribed 6 new aligners to complete alignment. Tooth whitening treatment was performed when the upper bonded retainer was fitted, using Opalescence 16% Carbamide Peroxide for two weeks at night. Finally, the composite edge bonding was performed on the LR1 and photos were taken.
Support and Mentorship
Working with IAS Academy makes you feel like you are not working alone. Ultimately, you are the clinician carrying out the treatment for the patient but help and advice is always close at hand. Throughout each stage of the treatment, I was able to post my progress on the online forum to ensure I was carrying out safe and effective treatment for my patient.
Reflection
The patient was very happy with the final result. I am happy with the outcome but have recently been introduced to IPR leaf gauges – if I were to do this case again I would have used these to determine the correct amount of IPR more accurately, which I find ensures a case progresses efficiently.
 Pre treatment smile right
Pre treatment smile right  Post treatment smile right
Post treatment smile right  Pre treatment smile left
Pre treatment smile left  Post treatment smile left
Post treatment smile left  Pre treatment retracted
Pre treatment retracted  Post treatment retracted
Post treatment retracted  Pre treatment right lateral
Pre treatment right lateral  Post treatment right lateral
Post treatment right lateral  Pre treatment left lateral
Pre treatment left lateral  Post treatment left lateral
Post treatment left lateral  Pre treatment upper occlusal
Pre treatment upper occlusal 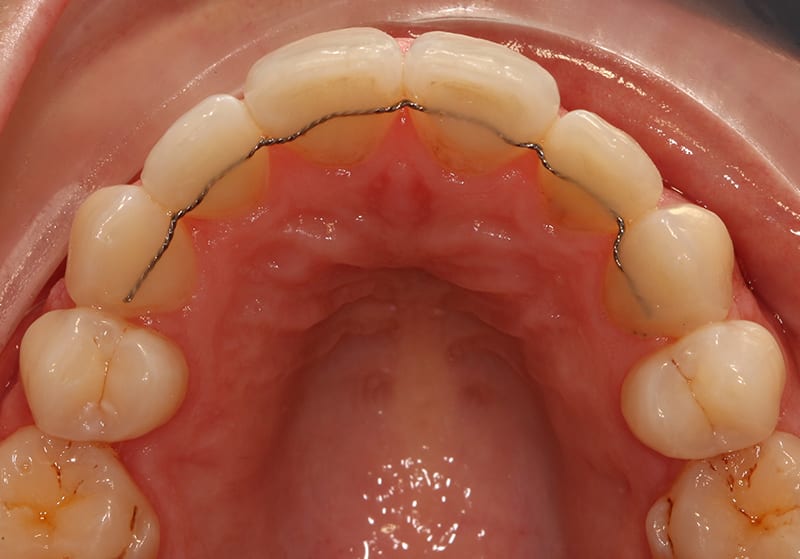 Post treatment upper occlusal
Post treatment upper occlusal  Pre treatment lower occlusal
Pre treatment lower occlusal 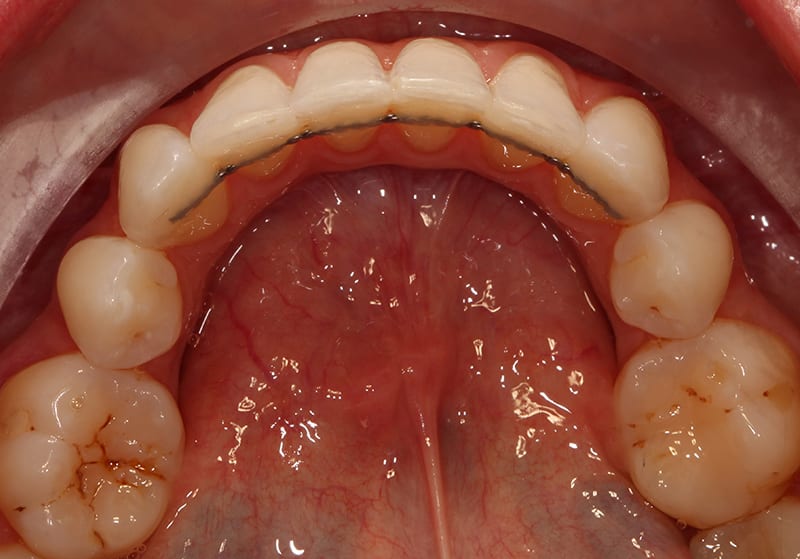 Post treatment lower occlusal
Post treatment lower occlusal 
