A Safer Way of Working

Treatment carried out by Utpalendu “Pinks” Bose
Utpalendu “Pinks” Bose MSc (Lond), DGDP(UK), LDSRCS(Eng) is a general dental practitioner (GDP) with a special interest in orthodontics. He owns and works in a general dental practice in Berkshire with particular predilection towards orthodontics for both children on the NHS and adults. He provides mainly conventional orthodontic treatment, but is also certified to provide aligner and lingual orthodontics. He strives to continually improve his orthodontic skills and was in the first cohort of the IAS Advanced Course under Professor Ross Hobson. He has since become an active member of the IAS team offering mentored support to like-minded GDPs keen to progress along the IAS Academy pathway.
Solid foundation for successful treatment
I am a GDP who has been practising conventional orthodontics for some time. In order to improve my practice I have attended several courses designed and targeted at GDPs throughout the UK. I found, while I picked up snippets of information along the way, I did not really get a satisfactory all-round exposure to the fundamental principles on the subject. I decided to attend the IAS Advanced course in 2015 under Professor Hobson and found that I had finally landed the course I had been craving to be on for years. There was enough theory to grasp the basic principles and apply these practically, safely and ethically through a carefully mentored programme in which you treat your patients (up to 20) under the direct and watchful supervision of a highly experienced clinician and academic. The whole process was to keep one safe and learn how to work within one’s scope of practice. Most importantly, you learn to recognise those cases that could pose problems and are best referred onto specialist colleagues or hospital consultants.
I learnt very quickly to do a full, thorough and complete orthodontic assessment, diagnose cases, and formulate a treatment plan – an ideal one, which is not always achievable, and a compromised version, which is often the way to approach a case. This is the core message of the course. As long as the assessment and diagnosis are correct, the planning is straightforward and treatment then starts to become second nature. The course is offered in modules with both theory and practical hands-on components. There was lot of emphasis on critical reading, journal club, learning to set up audits, undertaking these and deducing the results, interpreting radiographs used in orthodontic examinations, wire bending etc. Everyone had to present their cases – which was very helpful to me as I am not one for standing in front of people and talking. I had to learn how to use PowerPoint – I just wasn’t given the choice!
This presentation is a flavour of what kind of cases can be treated safely and confidently after taking this course.
Orthodontic records and assessment
A full orthodontic assessment was undertaken, diagnosis reached and treatment planned as a first step after obtaining pre-operative clinical photographs, a set of study casts and radiographs with the patient’s parents’ consent. The treatment plan included both ideal (including orthognathic surgery) and compromised aims focusing on full mouth treatment. The parents ruled out awaiting completion of growth and surgery (and therefore an ideal outcome) as an option, so it was agreed to proceed with the compromise plan. Had the parents opted for the ideal, the patient would have been referred to the Orthodontic Department at the local hospital.
Case summary
The case summary in brief was a healthy 14 year old girl with Class II division 2 incisal relationship on a mild skeletal II base with average vertical proportions, moderate crowding in the upper labial arch with contact point displacement of 4.5mm at UL23. There was mild crowding in the lower labial arch, no crossbites or mid-line displacement, ¼ Class II molar and canine relationships, an overjet of 3mm and an overbite of 90%. She had an Index of Treatment Need (IOTN) of 4d with an Aesthetic component of 5 and as such qualified for treatment under the NHS. (Figures 1-7)
Mentorship
The case was fully mentored by Professor Hobson right from the beginning. The completed comprehensive assessment form was submitted, along with appropriate high quality pre-operative digital photographs and radiographs where relevant. Professor Hobson’s approval was sought to start and finish the case. This involved a support portal – which everyone who has taken the course has full access to – where a complete photo series is uploaded at every visit, typically six weeks apart.
Treatment plan
The treatment plan was to undertake a compromised procedure (non-surgical) and accept the skeletal base, utilising upper and lower fixed appliances on a non-extraction basis.
A wire sequence of 0.012, 0.016, 20*20, and 19*25 NiTi wires was used to level, align and relieve the crowding.
Treatment finished with 19*25 stainless steel wires in the upper arch to express torque and 19*25 stainless steel wires with Reverse Curve of Spee (RCOS) in the lower arch to reduce the overbite.
Class II traction with 4.5oz*1/4” bands used bilaterally from the lower 6’s to the upper 3’s reduced the overjet. Based on the current literature, it can be stated that Class II elastics are effective in correcting Class II malocclusions, and their effects are primarily dentoalveolar. (5)
The patient was to have fixed retainers from teeth 3-3 in both arches with 0.175 Wildcat wire for life and Essix retainers at the end of treatment. (6,7)
Treatment
Treatment commenced in the upper arch only to avoid initial bracket interferences of the lowers. The sequence of wires was utilised as planned. Brackets (Evolve 0.22 MBT from DBO) were directly bonded free hand. Due to the deep overbite it was decided to start treating the upper arch and then commence treatment on the lowers once enough proclination of the upper teeth had been obtained to minimise the bracket interferences. (Figures 8-10)
Space was obtained for the lower brackets as the upper incisors responded to the treatment and splayed forward with proclination. The planned sequence of lower wires was undertaken and including 19*25 SS with RCOS at the lowers to reduce the overbite. (Figures 11-19)
Treatment concluded after 20 months and the patient and her mother were very happy with the result. (Figures 20-24)
Conclusions
All in all this was a really satisfying result. The treatment objectives were met with reduction of the overbite, correction of the overjet and achievement of a Class I relationship in the buccal segments. It demonstrates that a pleasing result need not always have to go through the ideal route.
What I took from this case was the importance of correct sequencing of the wires to complete treatment. The correct level of RCOS in a stainless steel wire was also necessary to get the best result.
Self critique
My critique of this case would be that, although a good overall result was achieved, the right side buccal segments could have been improved with the molars in a better interdigitated relationship. However, a lot of techniques were learnt, including correctly applying a reverse curve in SS wire to achieve a pleasing result. In hindsight I should have picked the lower 7’s as well, as this might have improved the buccal segments while also helping to reduce the overbite more efficiently and possibly reducing the overall treatment time. However, the patient and her mother were delighted with the result – the patient more so as she had the braces off in time for her prom!
I personally learnt, having attended the course and being closely mentored, that I need to think very carefully about what I am doing through a comprehensive assessment, diagnosis and plan. If in doubt, refer to the appropriate person. This one fact alone has changed my entire way of working in treating orthodontic patients.
 Pre Treatment
Pre Treatment  Pre Treatment
Pre Treatment  Pre Treatment
Pre Treatment  Pre Treatment
Pre Treatment  pre treatment upper
pre treatment upper 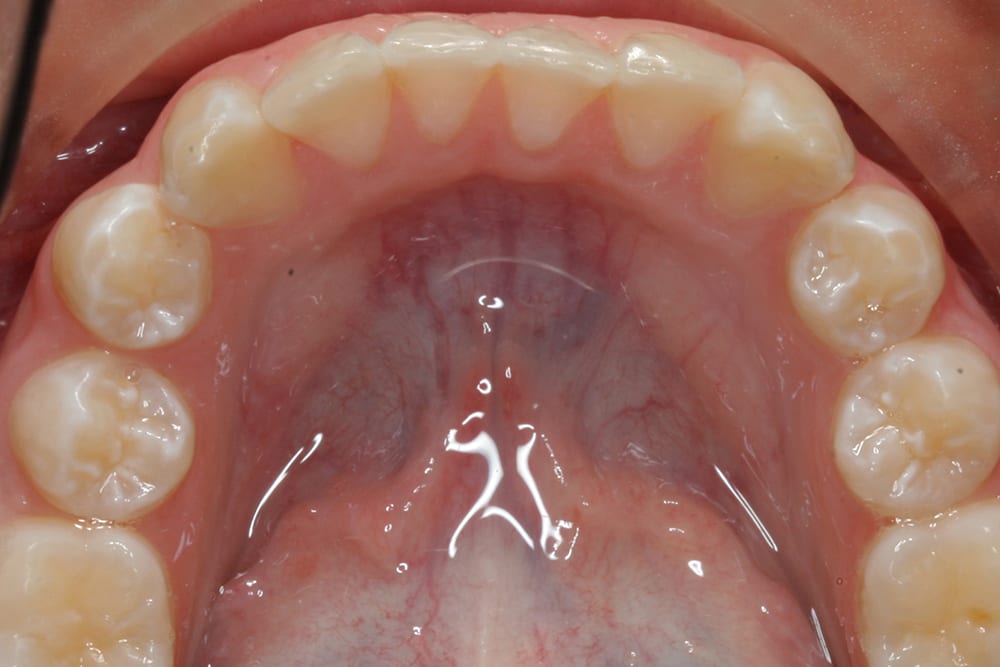 pre treatment lower
pre treatment lower  pre treatment retracted
pre treatment retracted  pre treatment left lateral
pre treatment left lateral  pre treatment right lateral
pre treatment right lateral  bond up 0.012 NiTi
bond up 0.012 NiTi  bond up 0.012 NiTi
bond up 0.012 NiTi  bond up 0.012 NiTi
bond up 0.012 NiTi  Mid treatment, upper archwire 19_25 SS, lower archwire 19_25 SS reverse curve of spee
Mid treatment, upper archwire 19_25 SS, lower archwire 19_25 SS reverse curve of spee  Mid treatment, upper archwire 19_25 SS, lower archwire 19_25 SS reverse curve of spee
Mid treatment, upper archwire 19_25 SS, lower archwire 19_25 SS reverse curve of spee 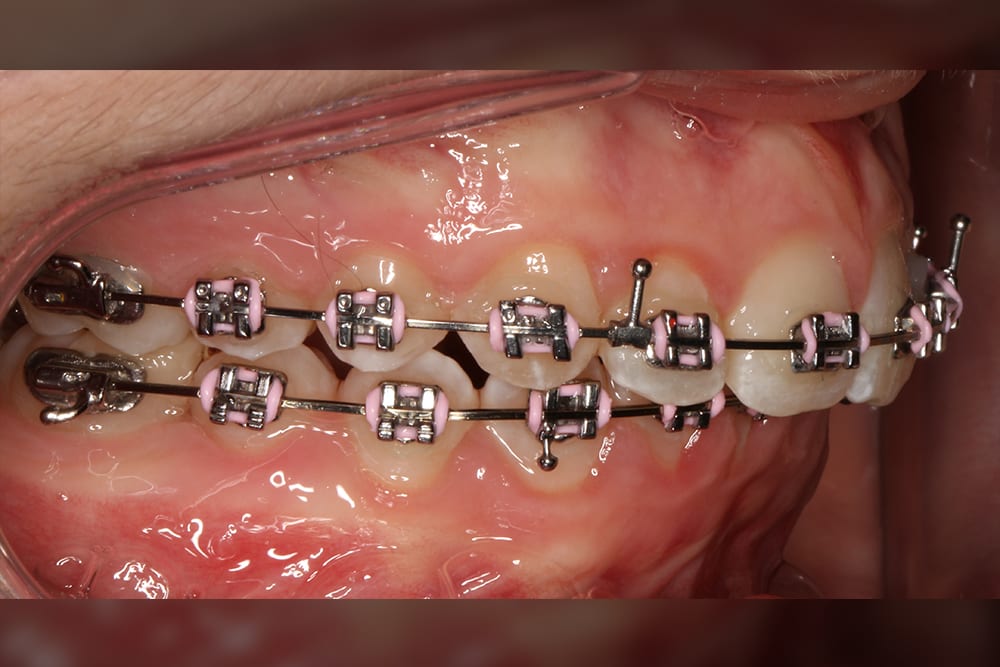 Mid treatment, upper archwire 19_25 SS, lower archwire 19_25 SS reverse curve of spee
Mid treatment, upper archwire 19_25 SS, lower archwire 19_25 SS reverse curve of spee  Mid treatment, upper archwire 19_25 SS, lower archwire 19_25 SS reverse curve of spee
Mid treatment, upper archwire 19_25 SS, lower archwire 19_25 SS reverse curve of spee 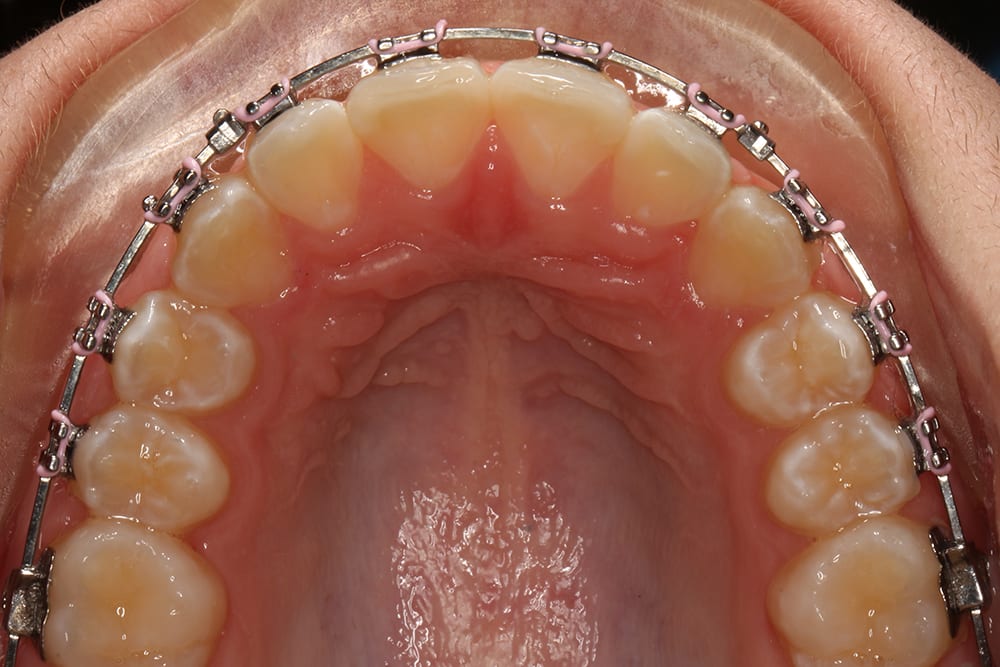 Mid treatment, upper archwire 19_25 SS, lower archwire 19_25 SS reverse curve of spee, upper occlusal
Mid treatment, upper archwire 19_25 SS, lower archwire 19_25 SS reverse curve of spee, upper occlusal  Mid treatment, upper archwire 19_25 SS, lower archwire 19_25 SS reverse curve of spee, lower occlusal
Mid treatment, upper archwire 19_25 SS, lower archwire 19_25 SS reverse curve of spee, lower occlusal  mid treatment in Class II traction 4.5oz_¼” bands (Orthocare) Full time wear bilaterally
mid treatment in Class II traction 4.5oz_¼” bands (Orthocare) Full time wear bilaterally  mid treatment in Class II traction 4.5oz_¼” bands (Orthocare) Full time wear bilaterally
mid treatment in Class II traction 4.5oz_¼” bands (Orthocare) Full time wear bilaterally  mid treatment in Class II traction 4.5oz_¼” bands (Orthocare) Full time wear bilaterally
mid treatment in Class II traction 4.5oz_¼” bands (Orthocare) Full time wear bilaterally  Post treatment
Post treatment  Post treatment right lateral
Post treatment right lateral  Post treatment left lateral
Post treatment left lateral 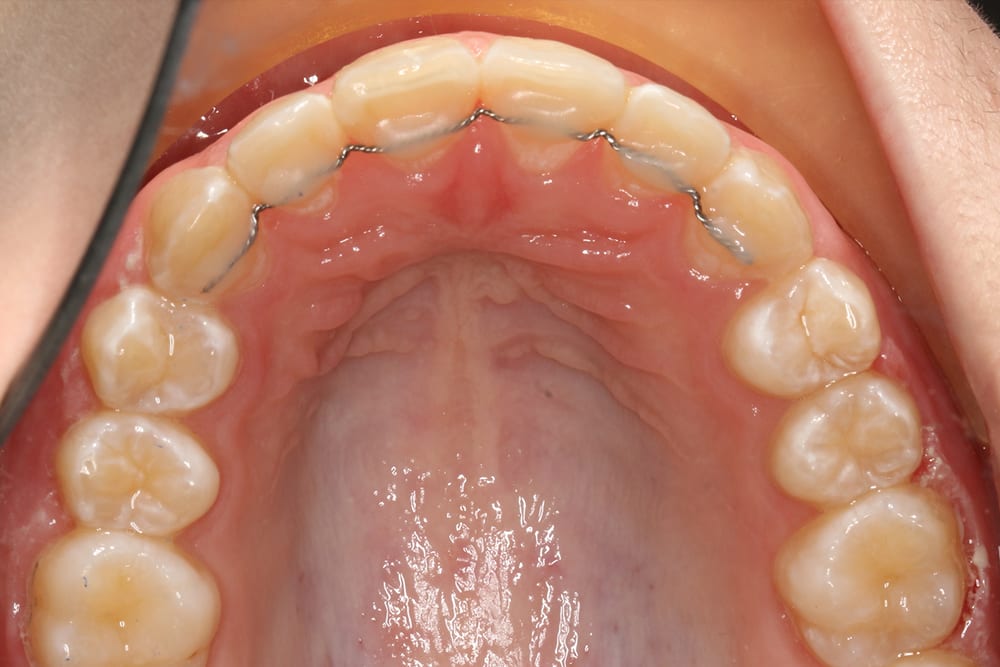 Post treatment upper occlusal with bonded retained
Post treatment upper occlusal with bonded retained  Post treatment lower occlusal with bonded retainer
Post treatment lower occlusal with bonded retainer  Post treatment
Post treatment  Post treatment
Post treatment  Post treatment
Post treatment  Post treatment
Post treatment  Post treatment
Post treatment 
